Community-Led Healthcare as Mental Health Infrastructure
How a community-led healthcare center in rural Rajasthan reached populations that no institution had served, and what the results reveal about the link between primary healthcare access and mental health.

In the Aravali belt of Rajasthan, more than 40 villages had no access to primary healthcare. The nearest hospital was 40 kilometers away. Preventable blindness, untreated chronic disease, and zero health records were the norm.
In July 2025, a community-led healthcare center called ARK (Arogya Raksha Kendra) opened in the village of Beejwa. Within seven months, it had served over 2,000 people, registered 1,166 patients with digital health records, conducted four specialist camps, and integrated telemedicine for remote consultations. Nearly half of all patients were women, in a region where social norms have historically kept women from accessing health services.
The model, developed by Dr. Ishan Shivanand, is formalized in Compassion Unites, a cross-sector mental health alliance.
40 Villages, Zero Access: The Rural Healthcare Gap in Rajasthan
Before ARK, the villages surrounding Beejwa had no local healthcare facility. The nearest hospital was in Alwar city, more than 40 kilometers away. For daily-wage families, the journey was prohibitive. The cost of consultation and medicine was out of reach entirely.
Cataract and glaucoma caused preventable blindness. The ARK team’s assessment found that nearly every household had at least two members with untreated eye conditions. Diabetes and hypertension went unmonitored. Children in local schools had never received a routine health assessment.
The consequences extend beyond physical health. When people cannot access basic care, treatable conditions become chronic. Chronic illness erodes the capacity to work, to care for family, to participate in community life. For women in particular, where social norms already restrict movement and autonomy, the absence of accessible healthcare compounds isolation.
The infrastructure gap was total: no physician, no pharmacy, no diagnostics, no health records, no pathway to specialist care, and no prospect of any.

How Community-Led Healthcare Delivery Works
ARK operates through four elements that Compassion Unites formalizes as a model for rural healthcare delivery. Three can be designed, funded, and deployed. The fourth, trust, already exists within communities. Compassion Unites activates it, connecting community hubs with medical expertise and technology to deliver healthcare where institutions have not reached.
Over 30 trained community members and a team of physicians and pharmacists deliver care at zero cost to patients. The community members, from non-medical backgrounds, were trained to deliver health support, manage patient flow, and operate diagnostic technology. This is a structured health delivery operation with professional medical oversight.
Specialist physicians rotate from across India: ophthalmologists from Bharatpur, pediatricians from Delhi, general surgeons from Jaipur and Alwar. The center operates seven OPD rooms, with specialist camps organized monthly. Physicians are scheduled 15 to 20 days in advance, covering different specializations on rotation. No permanent specialist staffing required.
ARK demonstrates what the Compassion Unites model calls activation: connecting sector expertise to community networks. The technology partnership with Wheels Global Foundation, working with IIT research teams, produced three platforms that form the backbone of care delivery:
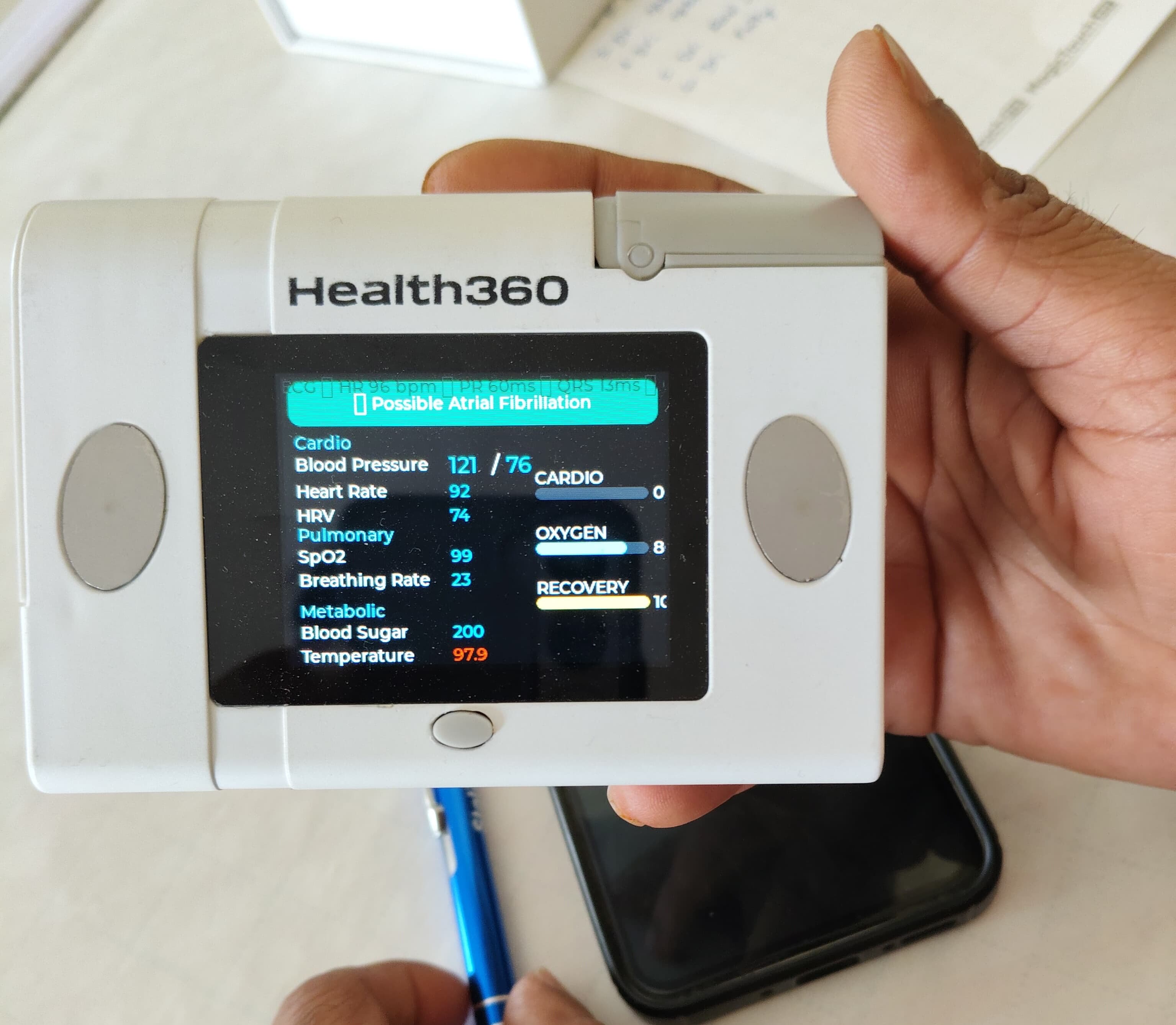
The Health360 device, a handheld multi-parameter screening tool measuring blood pressure, heart rate, HRV, SpO2, blood sugar, and temperature in a single assessment. Carried by volunteer teams into remote villages.
The My Smart Care Doc App, providing full digital patient records, symptom tracking, visit history, and follow-up scheduling. Deployed in March 2026, enabling population-level health data analysis for the first time in this region.
Telemedicine, connecting patients in Beejwa to specialist physicians anywhere in India via live video. Fully integrated as of March 2026.
Free care, specialist doctors, and good technology explain what ARK delivers. They do not explain why 47% of patients are women in a region where purdah is observed and where institutional health services have historically struggled to establish any presence.
The explanation is community trust. ARK was built within a network with deep roots in rural Rajasthan, established over 25 years through the ShivYog community’s service presence in Beejwa. When ARK’s team arrives with a community member in a village, they arrive within a relationship that already exists. Village heads endorse and support the center. School principals serve as health awareness ambassadors. Patients travel from well beyond the intended service radius.
Expertise, technology, and funding can be deployed, but trust cannot. Where trust exists, it unlocks outcomes that deployment-led models do not achieve: women showing up, families returning, entire villages treating the center as their own. And when women access healthcare for the first time, the impact extends far beyond the presenting complaint. A woman whose cataracts are treated can work again. A woman whose diabetes is monitored can care for her children. A woman who is seen and served by a healthcare system regains agency.
2,000+ Patients Across 40 Villages: Seven Months of Evidence
Between July 2025 and March 2026, ARK collected structured health data from a population that had never been documented. The numbers below represent the first comprehensive health profile of over 40 villages in the Aravali belt, and the first evidence of what community-delivered healthcare achieves when it reaches people for the first time.
ARK serves entire families, not a single demographic. The age distribution spans from infants to seniors over 60, reflecting a center that has become the primary healthcare touchpoint for whole communities. The 47% female patient rate is the standout figure: in a region where purdah restricts women’s movement, it signals a depth of community trust that clinical outreach programmes typically do not achieve.
The health burden profile reveals a population presenting with conditions that have gone untreated for years. Respiratory and eye conditions dominate because they are symptomatic: people come when they cannot breathe or cannot see. The “Other” category (23.7%) encompasses dental, ENT, gynecological, neurological, and infectious conditions, each individually small but collectively representing the broadest unmet need.
The low recorded rates of diabetes (3.8%) and hypertension (3.1%) are unlikely to reflect low prevalence. These are conditions that require screening to detect, and this population has never been screened. As ARK’s digital records and diagnostic capacity expand, the true chronic disease burden will surface.

Preventable Blindness in Rural India: From Screening to Surgery
Eye conditions are the second most common presenting complaint, and they reveal a pattern that defines the ARK model: once trust is established and primary care is accessible, patients come forward proactively with conditions they had previously accepted as inevitable. Across the region, preventable blindness from cataract and glaucoma has gone untreated for years. As ARK’s presence has grown, patients are now actively seeking diagnosis and surgical referral. The model creates, for the first time, a complete pathway from community screening to specialist diagnosis to surgical intervention, restoring not only sight but the capacity for independent living and economic participation.
What Happens When Communities Trust Their Healthcare
On 15 March 2026, ARK held its largest health camp. Over 400 patients from more than 30 villages were served in one day: blood pressure, blood sugar, and oxygen screening; pediatric consultations; eye examinations; and ARK’s first live telemedicine consultations with remote specialists. Free medicines were distributed to all attendees.
The camp demonstrated the model’s surge capacity. The same community trust that sustains daily OPD operations brought 400 people to a single event, from villages across the district.

Trust as a Referral Mechanism
The most significant finding from the community response is structural: the model generates its own demand. Patients now arrive from well beyond the intended service radius, including from other states, without any outreach campaign or marketing. Community trust functions as a referral mechanism. When people experience care and return to their villages, they bring others. Over 90% of surveyed patients reported a positive experience, but the stronger evidence is behavioural: families return, villages that were not in the original service area seek access, and local leaders actively integrate ARK into their own community infrastructure.
Primary Healthcare Access as a Mental Health Intervention
ARK addresses a root cause of poor mental health in underserved populations: the helplessness that comes from having no pathway to care. When a person is seen, diagnosed, treated, and followed up, they regain a measure of agency. That agency is protective.
The model is now expanding into direct mental health assessment. ARK has begun collecting baseline mental health data from children in rural schools surrounding Beejwa, combining physical health screenings with structured data collection on children’s wellbeing. The approach integrates lifestyle medicine, including nutrition guidance and wellness awareness, into a holistic assessment that trained community members can deliver.
With digital data capture through the My Smart Care Doc app, this assessment model can be deployed through over 1,000 ShivYog hubs across India simultaneously, generating mental health data from regions that have never been surveyed. It represents early intervention at its most fundamental: reaching children before conditions become clinical.
Scaling Community Healthcare: What the Model Requires
ARK’s results in Beejwa demonstrate a model that institutional investors and development partners can evaluate against a clear set of components. Each element has been tested over seven months of continuous operation, documented through digital health records, and designed for replication across geographies.
Purpose-built center with consultation rooms, reception, pharmacy, and accommodation for visiting physicians. The Beejwa facility operates seven OPD rooms.
Trained local people delivering health support, managing patient flow, and operating diagnostic technology under professional medical oversight. Recruited from within the community they serve.
Health360 devices for point-of-care screening, the My Smart Care Doc app for digital records and data analysis, and telemedicine for remote specialist consultations. Portable and deployable.
Specialist physicians connected to communities on a rotating basis. Expertise flows to where trust exists, covering multiple specializations without requiring permanent staffing at each site.
When healthcare is delivered by people from within a community, patients engage because the relationship already exists. Compassion Unites’ network of over 1,000 hubs across India provides this activation layer. The model requires equipping communities that already have trust with the expertise and tools to act on it.
Cost Structure: $3 to $6 Per Patient
ARK operates at a cost of $3 to $6 per patient. An initial facility investment covers construction, equipment, and technology platforms. Once operational, the center serves 500 to 1,000 patients per month. Four of the five components are standard health infrastructure: a facility, training, devices, and physician time. They are fundable, quantifiable, and deployable. The fifth, community trust, is the element that conventional health programmes spend years and significant outreach budgets trying to build. In this model, it already exists. Investment equips communities that already have trust with the expertise and tools to act on it. This fundamentally changes the cost structure and the timeline for impact.
Additional ARK centers are in development across India, with the Beejwa model serving as the operational blueprint.
Replicate This Model
To learn how the ARK model can be deployed in your community, request a conversation with the team. Our team can support you on this mission.